
Functional Range Conditioning (FRC): Where's the Research?
GH Note:
I attempted to get this paper published a few times, honestly I don’t want to go through the process of editing and formatting this for each different journal again. Instead, in line with my goal this year of open sourcing the information I’ve learned for the betterment of all coaches and therapists; here it is for you to read. While this isn’t Pubmed, I hope it is a start for those seeking answers.
A question that gets raised all the time is, if the system is great why is there no research. There are cited papers to show where the ideas are generated from, but even fellow certified practitioners continue to struggle with these concepts and ideas as it pertains to what is currently available research wise. Hence, this is where the idea for this paper was born. I suppose since it will live here on my website, it can be a living document I periodically update.
Gary
Editorial: Functional Range Conditioning (FRC): Where’s the Research?
Dr. Gary Heshiki, DPT, CSCS
Doctor of Physiotherapy, Certified Strength and Conditioning Specialist
No university affiliation
Sydney, NSW Australia
The author does not have any financial disclosure
No external funding received
The author states a conflict of interest as a certified FRC practitioner but does receive any financial benefit or funding through Functional Anatomy Seminars
Functional Range Conditioning (FRC) : Where’s the Research?
Abstract
Background: Functional range conditioning (FRC) is a mobility-strength training system created by Dr. Andreo Spina focusing on joint health optimization based on scientific principles and research (FRS1). Popularized over a decade ago, FRC has been presented to hundreds of professional sports teams and consulted with NASA. Despite the recognition FRC has gained, there is a dearth of direct research examining FRC within the strength and conditioning or rehabilitative fields.
Clinical Questions: What are relevant studies corroborating the usage of Controlled Articular rotations (CARs) and Progressive Angular Isometric Loading (PAILs) and Regressive Isometric Loading (RAILs)?
Key Results: A 2018 systematic review by Oranchuk et al (2018 23) examined the various effects of isometric exercise in varying joint angles. This review collated various trainable qualities encompassing the FRC system, including concepts from various adjacent scientific fields.
Clinical Application: Through the clinical adoption of CARs, coaches can confidently manage clients in a time-efficient and empowering methodology.
Key Words: FRC, Cars, Pails, Rails, isometrics, objective assessments, Physiotherapy, Functional Range Conditioning, mobility training, FRC mobility.
This commentary aims to help coaches and specialists connect the dots behind the principles of the FRC system in the hopes of future clinical research.
INTRODUCTION:
Clinicians working within a musculoskeletal setting use range of motion as a primary clinical outcome measure (Gajosik and Bohannon2). This is based on a rigid understanding of a joint’s degrees of freedom. We currently understand a shoulder to have three degrees of freedom (DOF), knees to have two, and so on as understood through arthrokinematics. This assumes looking at human movement only within the constraints of a rigid system. When examining adjacent fields of science, it is understood that the human body is a dynamic system with access to an infinite number of positions. This was originally proposed by Bernstein as a DOF problem (Bernstein3). When examining human movement as a system, we look at capacity as a measurable unit where we build from the inside to increase the system’s ability to undertake demands. This examines it as a system that has a global space in which it can work. For years, our understanding of DOF has been rigid to make it easier to study the function of a joint by reducing the variables to account for. When we substitute DOF for functional degrees of freedom (fDOF) we can focus on a non-linear view of human movement as a phase space that is made up of an infinite number of combinations for movement (Li4).
The rationale for an alternative MSK standard assessment of joint rotation is proposed. In human movement, each joint represents a single specific DOF. Life is inherently multidimensional, characterized by diverse movements in various planes. When analyzing what we traditionally consider as linear motions, the primary joints typically function through a combination rotational mechanisms. This prompts us to ask: When studying movement, where does one motion transition into another, such as horizontal abduction to full flexion? Our understanding of movement is currently defined by DOF, specifically altering joint positions to affect the DOF accessible to our bodies.
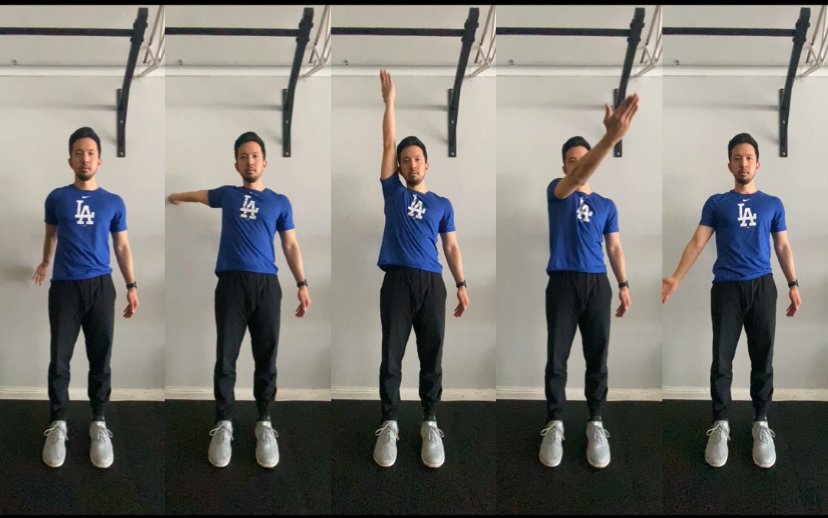
Introduced by Functional Anatomy Seminars, a CAR refers to an active, rotational movement performed at the outer limits of a joint's range of motion (ROM). Through CARs, FRC attempts to account for both rotational and transitional zones of movement. For instance, an individual progresses from a straight-line shoulder flexed position into abduction, then internally rotates to explore the outer limits of their active range of motion (ROM). This approach allows clinicians to gain a comprehensive view of an individual's fDOF and articular health.
Understanding CARs:
Our joint capsules contain specialized receptors such as Ruffini-like receptors, Golgi tendon organs in ligaments, and encapsulated Pancian-lie corpuscles. These mechanoreceptors are densely concentrated in regions associated with extreme movements, with capsular tissue serving as the primary sensory mechanism to detect these limits. They provide afferent information to the central nervous system (CNS), activating reflex mechanisms aimed at preventing injury (Zimny et al5). During a CAR, the muscle spindle undergoes stretching, transmitting sensory information to the CNS. This activity enhances alpha motor neuron function and helps maintain optimal length-tension properties (McGee6 Scholz and Campbell7).
During a CAR, the joint is moved through its full range, emphasizing end ranges of motion. This practice aligns with one of the fundamental principles of CARs, illustrating the effective transmission of afferent-efferent information between joint mechanoreceptors and the central nervous system (CNS). A CAR serves as an external indicator of the cortical action map, reflecting the brain's perception of spatial orientation based on sensory feedback. Changes in afferent information from peripheral joints are believed to precede neuroplastic changes in neural activation (Ward et al8).
When examining the glenohumeral joint (GHJ), it primarily consists of synovial cells, fibroblasts, and an extracellular matrix (ECM). The ECM is mainly type I collagen fibers in the superficial layers and type II and III collagen fibers in the deeper tissue layers. Type I mechanoreceptors are slow-adapting and primarily responsible for kinesthetic awareness (Cooper et al9). This is the histological pattern seen in the shoulder, hips, and neck, whereas the lumbar spine, hand, and feet primarily contain type II mechanoreceptors. This reinforces the idea that changes in areas of greater type I mechanoreceptors will require more frequent input to drive adaption.
Figure 1: From left to right, positions and transition zones of a shoulder CAR.

Figure 2: From left to right, positions and transitions zones returning through a shoulder CAR.
Capsular Assessment Through CARs
The posterior capsule limits posterior translation of the humeral head on the glenoid, and it tightens with glenohumeral joint (GHJ) internal rotation (IR) and GHJ horizontal adduction (HAD) (Hjelm et al10, Dashottar and Borstad11). Histological studies have shown that ligaments contain extensive populations of receptors, including Ruffini, Pacinian, and Golgi receptors (Duthon et al12, Zimny and Wink13, Zimny et al14)
A primary diagnostic use of CARs is examining if the restriction is a closing angle joint pain. If we understand GHJ IR and HAD to increase tension on the posterior capsule, it is surmised that if it is not able to accept the load, it will result in a closing angle joint pain eg: as one moves into internal rotation, you get pain anteriorly in the direction you are moving in. Similarly, we can attribute part of the closing angle joint pain experienced during end-range hip flexion to a possible lack of posterior translation of the femoral head within the acetabulum (Addison, D.E.15).
Using this information:
Building off the work of Stephen Levin and biotensgrity, a mechanical model, that takes into consideration the fascia line system (Bordoni and Meyers Thomas Meyers 16), FRC has coined a term called bioflow which is defined as a conceptual framework to understand the continuous nature of human movement and the tissues that produce it (FRS 1).
When we break down the system from a cellular level, first we understand that musculoskeletal muscle fibers are heterogenous and not homogenous. This is interpreted as fiber architecture made of short fibers in series as opposed to one long fiber running the length of attachment sites (Heron and Richmond 17). Based on this understanding of fiber architecture hierarchy, the gaps between these short fibers are filled in with connective tissue. Both Levin and Spina posit that connective tissue is not merely a passive structure but one that is involved in force production and transmission of said forces to be propagated through the system.
The work of Helene Langevin has been pivotal in the development of the FRC system as it confirms the importance of connective tissue within the human movement system. The linking of readily available research will serve as the foundation from which future research can investigate the system’s efficacy and validate FRC as a primary system that therapists might use to run their patients through. Langevin’s work centered around a change in conceptual understanding that the deformation of connective tissues to stretch demonstrated alpha and beta-actin response despite not being myofibroblastic cells. This explains how mechanotransduction and subsequent dynamic remodeling occur over time (Langevin et al 18-19). This serves as the foundation for the physiological changes that might explain the benefits of FRC’s second core modality, pails and rails.
Pails and Rails
These are isometric contractions, sometimes combined with stretching, used to communicate with both the connective tissue and neurological systems (FRS1). PAILs look to train articular angles to focus on articular strength at angles with the purported benefit of tissue adaptations at shorter tissue angles.
When reviewing stretch physiology, our current flexibility can be seen as our stretch tolerance. This is determined by your previous CNS experience and the ability of your muscles to function at a particular range (Magnusson et al 20). As we progressively increase the CNS ability to control new ranges of motion, we now effectively activate the greatest number of motor units via our understanding of overcoming isometrics (Thibaudeau 22). Current understanding within strength and conditioning (S&C) of the SAID principle can be applied not only to musculoskeletal tissue but all the enveloping tissues as they too contain contractile properties (Klinger et al 21). We can surmise that contractile proteins contain tensile properties and the ability to adapt to loads.
Key Result
Pails contractions are understood to be an overcoming isometric. The goal here is to contact the greatest amount of tissue on the lengthened side. Rails contractions are understood as an end-range active isometric contraction or a yielding isometric contraction. While the nomenclature suggests it’s an isometric, it is an active and persistent attempt at increasing tensile forces in the respective tissues (Thibaudeau 22).
A 2018 systematic review by Oranchuk et al (2018 23) examined the various effects of isometric exercise in varying joint angles. One aspect was comparing isometrics at short (SML) and long (LML) muscle lengths regarding muscle architecture. The vastus lateralis fascicle length at mid portion increased following short muscle length isometrics. Whereas LML increased distal fascicle length within the same muscle (Noorkoiv et al 24).
Tendon adaptations were investigated across six studies focusing on structural and functional changes. Notably, high-intensity isometric training led to significant increases in both Achilles tendon cross-sectional area and stiffness, whereas low-intensity training did not produce similar effects. A limitation of these studies was the narrow range of intensities examined, specifically at 55% and 90% of maximal voluntary isometric contraction, leaving a significant portion of the intensity spectrum unaddressed (Kubo et al 25).
Research suggests that long muscle length (LML) training favors morphological changes in the tendon. For instance, Kubo et al. examined knee extensors at 50 and 90 degrees of flexion, finding that training at the latter angle resulted in significant increases in tendon stiffness, as indicated by elongation of the distal tendon and aponeurosis. In contrast, short muscle length (SML) training led to only minor changes, supporting the conclusion that tendon adaptation can occur irrespective of muscle length during training. This underscores the idea that the greater load associated with long muscle contractions may contribute to positive tendon adaptations. All basic properties within the system of FRC in musculoskeletal training and therapy.
Currently in pre-publication by (Oranchuk et al27), a 2024 review highlights key principles regarding the use of isometrics in rehabilitation and training. The authors distinguish between two types of isometrics: "pushing" to represent overcoming isometrics (e.g., PAILs) and "holding" to represent yielding isometrics (e.g., RAILs).
The review emphasizes that yielding isometrics (holding patterns) tends to increase muscle activation with fewer neurological disturbances, particularly in joint pain. During yielding isometrics, there is an initial neurological activation followed by a sustained hold, which is less complex than the continuous adjustments required during isotonic movements. This balanced contraction reduces shearing forces across the joint, a principle that has been supported by its application in various injury management protocols.
Interestingly, most isometric protocols examined in the review focused on mid-range joint positions (90 deg), where resistance training commonly occurs. This positioning may influence the observed outcomes, as mid-range is associated with favorable joint mechanics and muscle recruitment. The authors also reported uneven distributions of effort between overcoming and yielding isometrics, noting that overcoming isometrics (pushing patterns) facilitates greater neurological adaptations.
A major drawback from this review is that the majority of studies (39/54) investigated intensities lower than 30% of intensity whereas a small amount (5/34) examined contractions up at 100% max voluntary isometric contraction intensity.
I propose that yielding or holding isometrics, which do not involve pushing against an external object, are inherently less stable and therefore less intense. This distinction may further explain differences in muscular and neurological responses between these two isometric strategies.
Clinical questions
Clinically this is a change from the traditional view of assessing movement to adopt a deeper, less empirical view of movement where one looks to remove a systems 1 approach to assessment (Tay et al26). Movement assessments come with drawbacks, primarily the inability to discern between aberrant tissue behavior and one that is related to motor control, e.g.: a poor squat does not equal a weak hip.
Clinical Application
When using CARs, breaking down the movement into positions and transition zones promotes inter-therapist consistency. Thereby improving therapist outcomes as an improvement in CARs can be seen as greater capsular tissue quality and increased workspace.
An overlooked benefit of running FRC to assess clients is the significant time savings. Traditional assessment methods require observing active motion before passive motion. Prioritizing efficient use of training time, the ability to evaluate a patient’s movement and identify dysfunctional joints without switching between active and passive assessments becomes highly relevant. This is especially important in a clinical environment where coaches frequently feel constrained by limited time for preventative care over performance training.
Finally, while CARs are a significant component of the FRC system, understanding that as a stand-alone exercise does a disservice to our patients. Without proper coaching and a thorough understanding by the coach of what they are observing, CARs could be no more effective than any randomly chosen movement.
Within the Functional Range System community, the question of research pops up, I hope that this commentary enhances practitioners' understanding of the FRC system and encourages others to investigate the effectiveness of FRC against standard traditional training models.
ACKNOLWEDGEMENTS:
The author is certified through Functional Range Systems but holds no direct financial ties to the organization.
REFERENCES
12.
B DV, Barea C, Abrassart S, H FJ, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surgery, Sports Traumatology, Arthroscopy. 2005;14:204-213. doi:https://doi.org/10.1007/s00167-005-0679-9
3.
Bernstein N. The co-ordination and regulation of movements. Brain Research. 1969;13:624. doi:https://doi.org/10.1016/0006-8993(69)90278-9
17.
Bordoni B, Myers T. A review of the theoretical fascial models: Biotensegrity, fascintegrity, and myofascial chains. Cureus. Published online February 2020. doi:https://doi.org/10.7759/cureus.7092
1.
Brunswick, M. Functional range Conditioning®. Functional Anatomy Seminars. https://functionalanatomyseminars.com/frs-system/functional-range-conditioning/
9.
Cooper C. Fundamentals of Hand Therapy : Clinical Reasoning and Treatment Guidelines for Common Diagnoses of the Upper Extremity. Elsevier Mosby; 2014:51-66.
11.
Dashottar A, Borstad J. Posterior glenohumeral joint capsule contracture. Shoulder & Elbow. 2012;4:230-236. doi:https://doi.org/10.1111/j.1758-5740.2012.00180.x
2.
Gajdosik RL, Bohannon RW. Clinical measurement of range of motion. Physical Therapy. 1987;67:1867-1872. doi:https://doi.org/10.1093/ptj/67.12.1867
5.
Harrison DE, Cailliet R, Betz JW, et al. A non-randomized clinical control trial of Harrison mirror image methods for correcting trunk list (lateral translations of the thoracic cage) in patients with chronic low back pain. European Spine Journal. 2004;14:155-162. doi:https://doi.org/10.1007/s00586-004-0796-z
16.
Hengeveld E, Banks K. Maitland’s Vertebral Manipulation : Management of Neuromusculoskeletal Disorders - Volume 1. Elsevier Health Sciences UK; 2013:375-449.
10.
Hjelm R, Draper C, Spencer S. Anterior-inferior capsular length insufficiency in the painful shoulder. Journal of Orthopaedic & Sports Physical Therapy. 1996;23:216-222. doi:https://doi.org/10.2519/jospt.1996.23.3.216
18.
I HM, J RF. In-series fiber architecture in long human muscles. Journal of Morphology. 1993;216:35-45. doi:https://doi.org/10.1002/jmor.1052160106
22.
Klingler W, Velders M, Hoppe K, Pedro M, Schleip R. Clinical relevance of fascial tissue and dysfunctions. Current Pain and Headache Reports. 2014;18. doi:https://doi.org/10.1007/s11916-014-0439-y
25.
Kubo K, Ohgo K, Takeishi R, et al. Effects of isometric training at different knee angles on the muscle-tendon complex in vivo. Scandinavian Journal of Medicine and Science in Sports. 2006;16:159-167. doi:https://doi.org/10.1111/j.1600-0838.2005.00450.x
19.
Langevin HM, Storch KN, Cipolla MJ, White SL, Buttolph TR, Taatjes DJ. Fibroblast spreading induced by connective tissue stretch involves intracellular redistribution of α- and β-actin. Histochemistry and Cell Biology. 2006;125:487-495. doi:https://doi.org/10.1007/s00418-005-0138-1
20.
Langevin HM, Storch KN, Snapp RR, et al. Tissue stretch induces nuclear remodeling in connective tissue fibroblasts. Histochemistry and Cell Biology. 2010;133:405-415. doi:https://doi.org/10.1007/s00418-010-0680-3
4.
Li ZM. Functional degrees of freedom. Motor Control. 2006;10:301-310. doi:https://doi.org/10.1123/mcj.10.4.301
27.
Oranchuk DJ, Nelson AR, Lum D, Natera AO, Bittmann FN, Schaefer LV. Pushing versus holding isometric muscle actions; what we know and where to go: A scoping and systematic review with meta-analyses. medRxiv (Cold Spring Harbor Laboratory). 2024 Nov 5;
6.
McGee S. Evidence-Based Physical Diagnosis. Elsevier Health Sciences; 2012.
26.
NOORKÕIV M, NOSAKA K, BLAZEVICH AJ. Neuromuscular adaptations associated with knee joint angle-specific force change. Medicine & Science in Sports & Exercise. 2014;46:1525-1537. doi:https://doi.org/10.1249/mss.0000000000000269
24.
Oranchuk DJ, Storey AG, Nelson AR, Cronin JB. Isometric training and long-term adaptations: Effects of muscle length, intensity, and intent: A systematic review. Scandinavian Journal of Medicine & Science in Sports. 2019;29:484-503. doi:https://doi.org/10.1111/sms.13375
21.
P MS, B SE, Aagaard P, Sørensen H, Kjaer M. A mechanism for altered flexibility in human skeletal muscle. The Journal of Physiology. 1996;497:291-298. doi:https://doi.org/10.1113/jphysiol.1996.sp021768
7.
Scholz JP, Campbell SK. Muscle spindles and the regulation of movement. Physical Therapy. 1980;60:1416-1424. doi:https://doi.org/10.1093/ptj/60.11.1416
15.
Tay SW, Ryan PM, Anthony RC. Systems 1 and 2 thinking processes and cognitive reflection testing in medical students. Canadian Medical Education Journal. 2016;7:e97-103. doi:https://doi.org/10.36834/cmej.36777
23.
Thibaudeau C. Theory and Application of Modern Strength and Power Methods. CreateSpace; 2014.
8.
Ward S, Pearce AJ, Pietrosimone B, Bennell K, Clark R, Bryant AL. Neuromuscular deficits after peripheral joint injury: A neurophysiological hypothesis. Muscle & Nerve. 2015;51:327-332. doi:https://doi.org/10.1002/mus.24463
14.
Zimny ML, Schutte M, Dabezies E. Mechanoreceptors in the human anterior cruciate ligament. The Anatomical Record. 1986;214:204-209. doi:https://doi.org/10.1002/ar.1092140216
13.
Zimny ML, Wink CS. Neuroreceptors in the tissues of the knee joint. Journal of Electromyography and Kinesiology. 1991;1:148-157. doi:https://doi.org/10.1016/1050-6411(91)90031-y